|
BETTS
Glossary of Terms
|
Term
|
Definition and explanation |
| Eyewall |
Sclera and cornea.
| Though technically the eyewall has three coats posterior to the limbus, for clinical and practical purposes violation of only the most external structure is taken into consideration |
|
| Closed globe injury |
No full- thickness wound of eyewall. |
| Open globe injury |
Full- thickness wound of the eyewall. |
| Contusion |
There is no (full- thickness) wound.
| The injury is either due to direct energy delivery by the object (e. g., choroidal rupture) or to the changes in the shape of the globe (e. g., angle recession) |
|
| Lamellar laceration |
Partial- thickness wound of the eyewall. |
| Rupture |
Full- thickness wound of the eyewall, caused by a blunt object.
| Since the eye is filled with incompressible liquid, the impact results in momentary increase of the IOP. The eyewall yields at its weakest point (at the impact site or elsewhere; example: an old cataract wound dehisces even though the impact occurred elsewhere); the actual wound is produced by an inside- out mechanism |
|
| Laceration |
Full- thickness wound of the eyewall, caused by a sharp object.
| The wound occurs at the impact site by an outside- in mechanism |
|
| Penetrating injury |
Entrance wound.
| If more than one wound is present, each must have been caused by a different agent |
|
| Retained foreign object/ s. |
| Technically a penetrating injury, but grouped separately because of different clinical implications |
|
|
| Perforating injury |
Entrance and exit wounds.
| Both wounds caused by the same agent |
|
*Some injuries remain difficult to classify. For instance, an intravitreal BB pellet is technically an IOFB injury. However, since this is a blunt object that requires a huge impact force if they enter, not just contuse, the eye, there is an element of rupture involved. In such situations, the ophthalmologist should either describe the injury as “mixed” (i. e., rupture with an IOFB) or select the most serious type of the mechanisms involved.
Discussion
Worldwide interest in ocular trauma is rapidly growing as increasingly effective techniques for
prevention and treatment are developed. Professional associations (International Society of Ocular Trauma,
United States Eye Injury Registry) have been formed to promote research and disseminate its results.
Unfortunately, the lack of an unambiguous common language remains a major limiting factor in effectively
sharing eye injury information: varying responses are given to simple questions such as, What is the distinction between laceration, rupture, penetration, and perforation? Is a full- thickness scleral wound without obvious choroidal and retinal involvement an open globe injury? If a foreign body has traversed the eye and lodged in the orbit, is it perforating? double perforating? double penetrating? ).
Despite these ambiguities, whether publishing in a peer- review journal or discussing patient referral over
the telephone, ophthalmologists continue to use certain ocular trauma terms, rather than lengthy descriptions, to characterize the eye’s condition. Our colleagues‘ definition and understanding of these terms are assumed
identical to ours with each term having a definition which is unambiguous and independent of such variables as time, individuality, geographical location, and place of training. It is also commonly assumed that a one-to-one relationship between condition and term exists: there is no condition which can alternatively be described by more than a single term, and there is no term characterizing more than a single clinical condition. Unfortunately, our review of scientific journals and reference books proved these assumptions to be incorrect.
Without a standardized terminology of eye injury types, it is impossible to design projects like the United
States Eye Injury Registry (USEIR) or the World Eye Injury Registry (WEIR); clinical trials in the field of ocular trauma cannot be planned; and the communication between ophthalmologists remains ambiguous. A
standardized terminology for eye injury has been developed based on extensive experience. It has then
undergone repeated reviews by international ophthalmic audiences, incorporating suggestions from
respondents in 13 countries and selected ocular trauma experts. By always using the entire globe as the tissue of reference, classification is unambiguous, consistent, and simple. It provides definitions for the commonly used eye trauma terms within the framework of a comprehensive system.
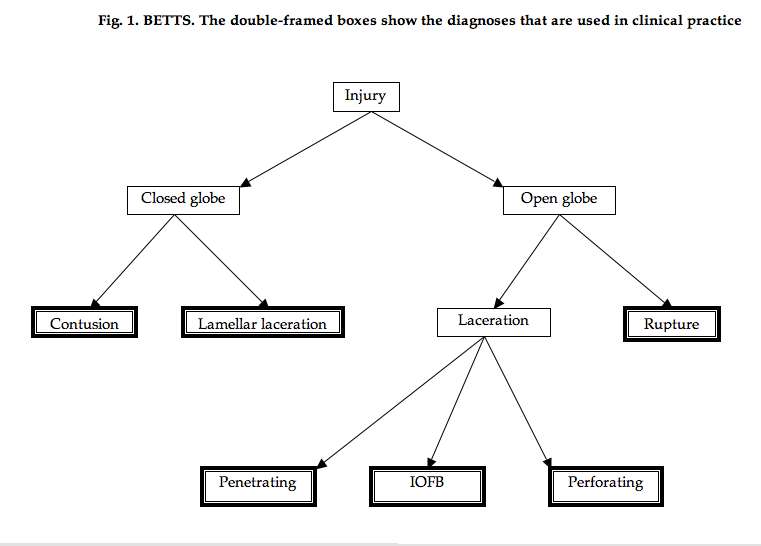
BETTS
BETTS satisfies all criteria by:
1) providing a clear definition for all injury types (Table 1)
2) placing each injury type within the framework of a comprehensive system (Fig. 1). The key to BETTS’ logic is to understand that all terms relate to the whole eyeball as the tissue of reference . While in BETTS, a “penetrating corneal injury ” is unambiguously an open globe injury with a corneal wound, the same term had two potential meanings before:
A. an injury penetrating into the cornea (i. e., a partial- thickness corneal wound: a closed globe injury) or
B. an injury penetrating into the globe (i. e., a full- thickness corneal wound: an open globe injury).
You can download a printable copy of this document in our downloads section of this website under the BETTS heading. |